

Tokaimura Nuclear Accidents
Japan’s Tokaimura nuclear accidents refer to two major incidents near Tōkai village, Ibaraki Prefecture. The 1997 fire at a bituminization facility exposed workers to radiation—but it wasn’t catastrophic. The far more devastating event occurred on September 30, 1999, at a facility operated by Japan Nuclear Fuel Conversion Co. (JCO). Technicians bypassed approved procedures and directly poured enriched uranium solution into a precipitation tank, triggering an uncontrolled 20-hour criticality reaction. Over 600 people were exposed; two workers died—including Hisashi Ouchi—and one survived minor radiation sickness.
Regulatory failures—lack of proper oversight, poor safety culture, and inadequate training—were major contributors. JCO’s unauthorized method using stainless steel buckets virtually eliminated all engineered safety design meant to prevent criticality.
How Much Radiation Did Ouchi Receive?
Hisashi Ouchi, aged 35, was the ethanolically unfortunate technician closest to the reaction when it went critical. Estimates indicate he absorbed approximately 17 sieverts (Sv) of radiation—well above the 4–5 Sv considered fatal. Those nearby, like Masato Shinohara, absorbed 10 Sv, and their supervisor Yutaka Yokokawa absorbed about 3 Sv.

This is Hisashi Ouchi’s photo. Credit: Peaked Interest YouTube Channel
Higher doses deliver massive bursts of neutrons and gamma radiation, instantly destroying cells and halting production of new blood cells. Ouchi’s bone marrow was eliminated, his lymphocyte count dropped nearly to zero, and his fate was effectively sealed within minutes.
What Does a High Dose of Radiation Do to the Body?
A high dose—especially instantaneous as in a criticality event—obliterates cells and DNA, cripples the immune system, and destroys skin, gastrointestinal lining, and internal organs. Within hours, symptoms appear: vomiting, diarrhea, dehydration, and redness of skin. Over days and weeks, blistering, ulceration, and massive fluid loss occur.
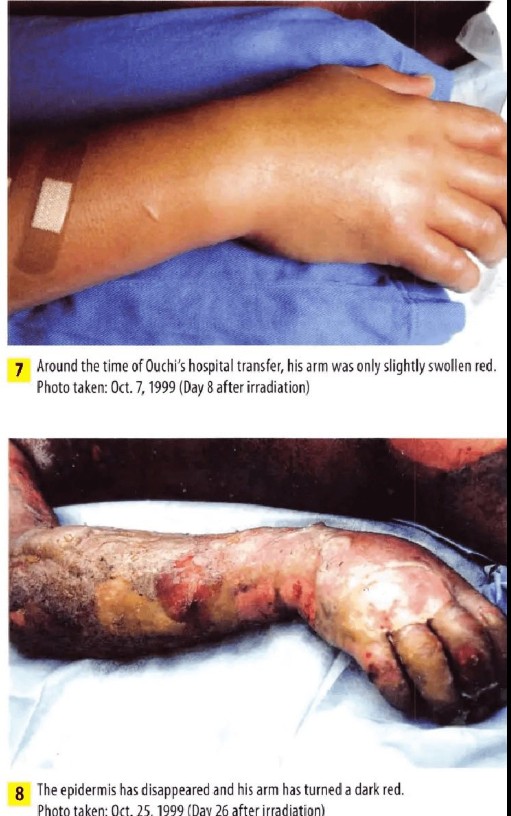
Radiation burns, or cutaneous radiation syndrome (CRS), can begin with redness and progress through blistering, peeling, and complete skin loss. In extreme exposures, the skin’s vascular network collapses after weeks. Hisashi Ouchi experienced almost full-body epidermal degeneration.
Ouchi’s Condition Continued to Deteriorate
After absorbing around 17 Sv of radiation—the highest recorded dose for a human being—Hisashi Ouchi faced catastrophic destruction of his bone marrow and immune system. Within hours, his lymphocyte count was nearly zero, signifying complete immune collapse. He vomited violently, suffered dehydration, and lost coherent consciousness.
Over the next days, his skin began peeling off under adhesive tape, revealing raw, exposed dermis. Toward the end of the first week, nearly all epidermal layers had sheared away, exposing tissue that oozed fluids by the liter. Stem cell engraftment showed early signs but failed—donor cells were as radiation-damaged as his own chromosomes. Doctors reported his chromosomes had become “unidentifiable”—shattered beyond recognition.
By the third week, his body produced little to no new immune cells, making infection inevitable. Gastrointestinal syndrome set in with relentless diarrhea, nutrient loss, and daily blood transfusions as his body hemorrhaged internally. Mold colonized his wounds, grafts slipped off, and internal organs began failing. He experienced multiple organ deterioration—kidney, liver, lung—each compounding the systemic collapse.
Around Day 59, he suffered three cardiac arrests within an hour, each time revived at his family’s insistence. The medical team was torn: his suffering was immense, yet his family demanded continued efforts, hoping he would make it to the year 2000.
What Exactly Happened to Hisashi Ouchi?
This is Hisashi Ouchi’s photo. Credit: Peaked Interest YouTube Channel
-
Date & Event: On 30 September 1999, at ~10:35 AM, technicians bypassed approved safety procedures and manually poured uranium solution into a precipitation tank, reaching critical mass. A blue-white flash of Cherenkov radiation marked the uncontrolled chain reaction that persisted for nearly 20 hours.
-
Exposure: Ouchi was at the tank holding a funnel when it went critical and received 17 Sv. His colleagues got lower doses: Masato Shinohara received ~10 Sv; Yutaka Yokokawa ~3 Sv and survived with mild radiation sickness.
-
Medical Response: Ouchi was initially sent to the National Institute of Radiological Sciences in Chiba, then transferred three days later to the University of Tokyo Hospital for advanced care—the only viable option for extreme radiation victims.
Hisashi Ouchi After Radiation: Skin, Injuries, Eyes
Skin & Soft Tissue Damage
His cutaneous radiation syndrome (CRS) progressed from reddening to blistering to full-thickness necrosis. Adhesive dressings peeled away flesh, leaving wide areas of raw tissue weeping fluids. Skin grafts—both cultured and from donors—were repeatedly tried but failed to adhere due to the compromised cellular environment.
Eye & Mucosal Effects
His eyes reportedly leaked blood, a sign of vascular breakdown. Multiple mucous membranes (oral, gastrointestinal) ulcerated and bled, heightening infection risk and severely impairing his nutrition and breathing capacity.
Internal Organs
High-dose radiation swiftly destroyed rapidly dividing cells—including those in bone marrow, gastrointestinal lining, and lungs. His liver enzymes skyrocketed (GOT ~3310, GPT ~1066), and kidney function collapsed, forcing continuous dialysis. Pulmonary damage undermined his respiratory stability, and mold colonization of wounds further complicated his condition
What Are the Side Effects of Hisashi Ouchi?
This is Hisashi Ouchi’s photo. Credit: Facebook
His ordeal encompassed nearly all major categories of acute radiation syndrome (ARS):
-
Hematopoietic syndrome: Bone marrow failure left him with zero white blood cells, severe anemia, and inability to clot—leading to internal bleeding and sepsis risk.
-
Cutaneous syndrome: Massive skin necrosis, blistering, ulceration, and inability to heal, resulting in fluid loss and open wounds.
-
Gastrointestinal syndrome: Severe diarrhea, vomiting, ulceration, and nutrient depletion leading to malabsorption and electrolyte imbalance.
-
Neurovascular involvement: At the lethal dose level (17 Sv), neurological degeneration was rapid; dizziness and decreased consciousness followed almost immediately—death was inevitable without miraculous intervention.
Physically, he endured continuous pain, vomiting, dehydration, hemorrhage, infections, cardiac crises, and relentless multi-organ failure. Psychologically and emotionally, he reportedly cried out, “I can’t take it anymore, I am not a guinea pig,” as experimental treatments continued against his will.
Who Was the Most Radiated Man in History?
Hisashi Ouchi holds the grim record for the highest radiation exposure ever documented in a human survivor—17 Sv, approximately equivalent to doses experienced by survivors of atomic bombs or Chernobyl workers—but at a recorded fatal level. His case remains unparalleled in both exposure and the duration of survival post-exposure.
Masato Shinohara, exposed to ~10 Sv, survived several months thanks to umbilical cord blood transfusion and aggressive treatment, but eventually succumbed in April 2000. Yutaka Yokokawa received ~3 Sv and recovered after three months, with minor effects.
Medical Interventions Attempted
Peripheral Blood Stem Cell Transplant
From Day 2–3, Ouchi’s bone marrow was found to be catastrophically damaged, with lymphocyte counts plummeting to as low as ~100‑300 cells/mm³—virtually zero immunological function. The team determined his chromosomes had been shattered and immune recovery without intervention was impossible .
An experimental peripheral blood stem cell transplant (PBSCT) was initiated using his sister as donor. She received mobilizing drugs to harvest stem cells via vein, a procedure chosen over traditional bone marrow transplant for faster white blood cell engraftment (10–14 days rather than weeks) and lower surgical risk.
By Day 17 (Oct 16), Ouchi’s WBC count rose to ~1000/mm³, and by Day 18, chromosome analysis showed engraftment of female (sister’s) cells—marking a rare medical success. Yet, donor cells quickly succumbed to residual radiation damage, ending any lasting marrow recovery.
Skin Grafts, Fluids & Blood Transfusions
From Days 8–21, radiation burns caused blistering and full-thickness skin loss. Adhesive dressings detached flesh, and his torso drained over 2 liters of fluid per day. Dozens of blood transfusions—often more than 20 daily—were needed to manage hemorrhage and anemia.
Multiple skin graft attempts—including cultured allografts from tissue banks and his sister’s cells—were tried between Days 22–49. Nearly all grafts failed due to constant fluid seepage and inability of his tissue to support regeneration.
Pharmacological Support & Organ Support
Broad-spectrum antibiotics aimed to combat infection in lieu of immune defenses. Granulocyte colony-stimulating factor (G-CSF) and erythropoietin/thrombopoietin were administered to stimulate blood cell production. Pain medication was heavy, sedation deepening as respiratory and organ failure set in .
By Day 60, his liver enzymes (GOT ~3,310, GPT ~1,066) indicated liver failure, while kidneys were failing and required continuous dialysis. Respiratory collapse necessitated intubation and ventilator care.
Specialist teams (from U.S., Russia, France, Germany) were called in—including Dr. Fred Mettler—to consult. Discussions included amputating necrotic limbs, but risk of non-healing wounds precluded it.
Final Decline and Death
By Day 59, Ouchi suffered three cardiac arrests in one hour; each time he was revived per his family’s wishes. He entered a coma, brain activity minimal.
On Day 81, doctors advised halting resuscitation; the family consented, hoping he might survive to New Year 2000. On Day 83 (December 21, 1999, at 11:21 pm), his heart failed irreversibly—his body succumbing to overwhelming multi-organ failure.
Ethical Dilemmas
Balancing Hope Against Suffering
The medical team faced intense moral questioning: Was it worthy to prolong life when recovery was medically implausible? Ouchi endured excruciating pain, daily wounds, repeated graft failures, and multiple resuscitations. Yet, his family’s steadfast demand for continued treatment raised complex issues of autonomy, hope, and dignity .
His reported plea—“I can’t take it anymore, I am not a guinea pig”—highlighted his psychological anguish and the ethical tension between experimental medicine and palliative care.
Informed Consent Under Trauma
Consent was difficult. Ouchi was sedated, semi-conscious, with no real capacity to understand or refuse. His family made decisions under trauma and hope. Ethical norms demand fully informed consent—impossible under these circumstances. The situation forced the medical team to balance professional obligations and respect for human dignity.
Medical Futility and End-of-Life Decision
By Day 59, with irreversible brain injury and no biological possibility for recovery, physicians recommended a do-not-resuscitate order. Family consent followed—raising questions about timing, transparency, and limits of life-sustaining treatment in experimental contexts .
Lessons Learned and Lasting Impact
Advancing Radiation Emergency Medicine
Ouchi’s case marked the first-ever use of peripheral blood stem cell transplantation for severe radiation injury—a breakthrough though not curative. It pushed boundaries in emergency hematology and offered invaluable data for future protocol.
Tightening Nuclear Safety Protocols
The Tokaimura disaster exposed severe gaps: safety shortcuts, wrong use of buckets, insufficient oversight, and lack of criticality alarms. In response, Japan revoked JCO’s license, prosecuted officials, and reformed safety culture—strengthening regulation and emergency preparedness nationwide.
Ethical Reflection in Medicine
The case underscored the challenges of treating extreme injury. It galvanized discussions in medical ethics about experimental treatment limits, patient autonomy when incapacitated, and recognizing when continuing care becomes cruelly futile—even at the behest of family .
A Human Reminder
Ouchi’s story remains a stark testament to the human cost of radiation disasters. Graphic hospital images, while ethically fraught, have served as cautionary visuals in training and policy discussions—reminding societies that negligence in nuclear industries can unleash human suffering beyond comprehension.
Masato Shinohara’s Parallel Case
Masato Shinohara, aged around 40, was one of the two technicians exposed to a near‑lethal dose during the Tokaimura criticality on September 30, 1999. He absorbed approximately 10 Sv—enough to guarantee death in most cases—while Yutaka Yokokawa received about 3 Sv and survived.
Unlike Hisashi Ouchi, Shinohara received an umbilical cord blood transplant, a novel approach at the time—an HLA‑mismatched graft intended to boost his depleted immune system as a bridge to eventual autologous marrow recovery IAEA. He survived for seven months, undergoing aggressive cancer‑style treatments, repeated skin grafts, and intensive infection control efforts. Despite this, persistent sepsis, lung and kidney failure eventually proved fatal; he passed away in April 2000.
Both men were initially saved by mechanical life‑support and experimental therapies, but Shinohara’s case illustrates that even with pioneering treatments he could not overcome the systemic damage wrought by such a high dose. While Ouchi suffered arguably the highest sustained dosage reported, Shinohara’s survival beyond two months offered key data for emergency medicine protocols.
Comparisons with Chernobyl Victims
While the Tokaimura accident was acute and localized, the Chernobyl disaster (April 26, 1986) involved a large-scale reactor explosion and widespread exposure. Victims of Chernobyl suffered various forms of acute radiation syndrome (ARS), but typically with lower radiation doses spread over time rather than the instantaneous extreme exposures seen at Tokaimura.
At Chernobyl, out of approximately 134 identified ARS cases, 28 died within months. Most received lower-dose exposure than Ouchi (17 Sv) or Shinohara (10 Sv), and typically experienced a shorter clinical timeline. Tokaimura thus stands out not only for maximal dosage but also the protracted, agonizing survival with full medical support—unparalleled in previous radiation accidents.
Broader Shifts in Radiation Emergency Protocols After Tokaimura
Revised Medical Response Practices
Tokaimura’s extreme cases spurred major enhancements in radiation emergency medicine:
-
Use of peripheral blood stem cell and cord blood transplantation as acute-phase interventions—with better donor matching, preparation, and ethical oversight.
-
Improved infection prophylaxis and wound-care for patients with total bone marrow failure.
-
Creation of specialized radiation treatment wards to limit infection risk and centralize care.
Institutional and Regulatory Reform
Regulatory bodies in Japan and internationally moved quickly:
-
JCO’s license was revoked, six executives were prosecuted, and judicial reforms mandated strict inspections and accountability in nuclear operations.
-
The incident prompted mandatory installation of criticality alarms, stricter operator qualification standards, and emergency planning at all nuclear facilities.
-
Widespread organizational change fostered a safety culture emphasizing compliance and incident prevention.
Ethical and Operational Guidelines
The crisis unveiled limitations in existing protocols for consent and end-of-life decisions under catastrophic injury:
-
Institutions now emphasize early ethical consultation, palliative care integration, and advance directives, especially in irreversible cases.
-
Training programs for radiation emergencies incorporate informed consent under duress, realistic expectation setting, and psychological support for families and staff.
Summary Table: Tokaimura vs. Chernobyl
| Feature | Tokaimura (1999) | Chernobyl (1986) |
|---|---|---|
| Exposure Type | Acute, localized criticality | Mixed acute & chronic environmental exposure |
| Maximum Dose Experienced | ~17 Sv (Ouchi) | Typically <10 Sv for most ARS fatalities |
| Duration of Survival | Ouchi: 83 days; Shinohara: ~7 months | Many died within weeks to months (28 confirmed ARS deaths) |
| Experimental Medical Response | Stem cell & cord blood transplants, grafts | Supportive care only (stem-cell therapy rare) |
| Ethical Challenges | Informed consent, experimental limits | Less protocol for mass casualties or delayed consent issues |
| Institutional Outcome | Shutdown, prosecutions, regulatory overhaul | Broader USSR response; long-term cleanup protocols |
Tokaimura’s tale remains one of the gravest lessons in nuclear safety and medical ethics. Ouchi and Shinohara’s suffering yielded deep knowledge about human limits under extreme radiation, while spotlighting the necessity of stringent oversight, operator training, and ethical clarity when intervention may inflict more pain than it relieves.
Featured Hisashi Ouchi Photos Credit: Facebook
Disclaimer: All images used in this guide are sourced from various YouTube channels and Social Media and are included solely for informational purposes. Full credit and rights belong to their respective owners.